Rare comminuted fracture in the elbow joint
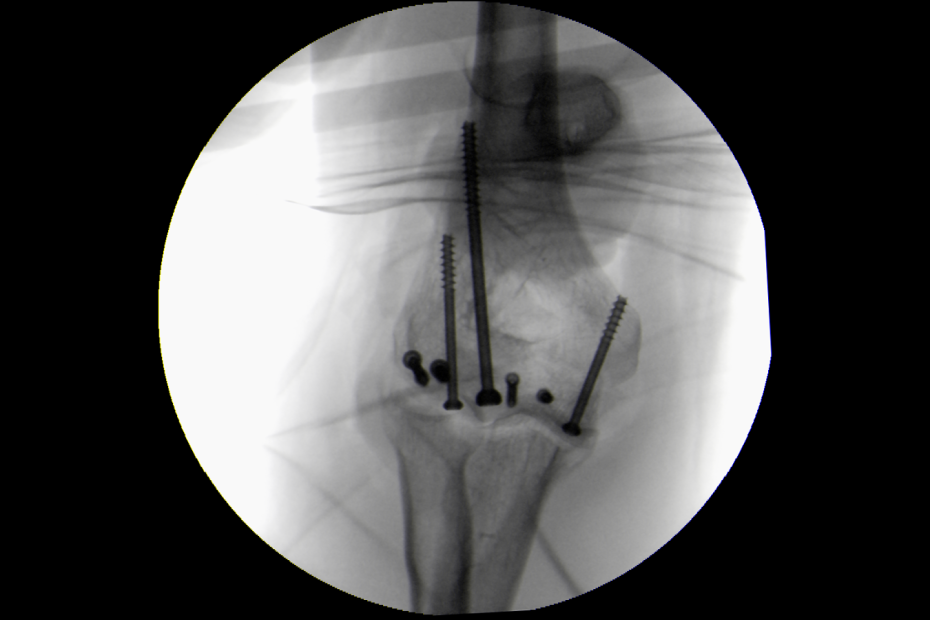
Comminuted fractures of the elbow are very difficult to treat. The X-rays show the bone reconstruction procedure from start to finish.
Comminuted fractures of the elbow are very difficult to treat. The X-rays show the bone reconstruction procedure from start to finish.
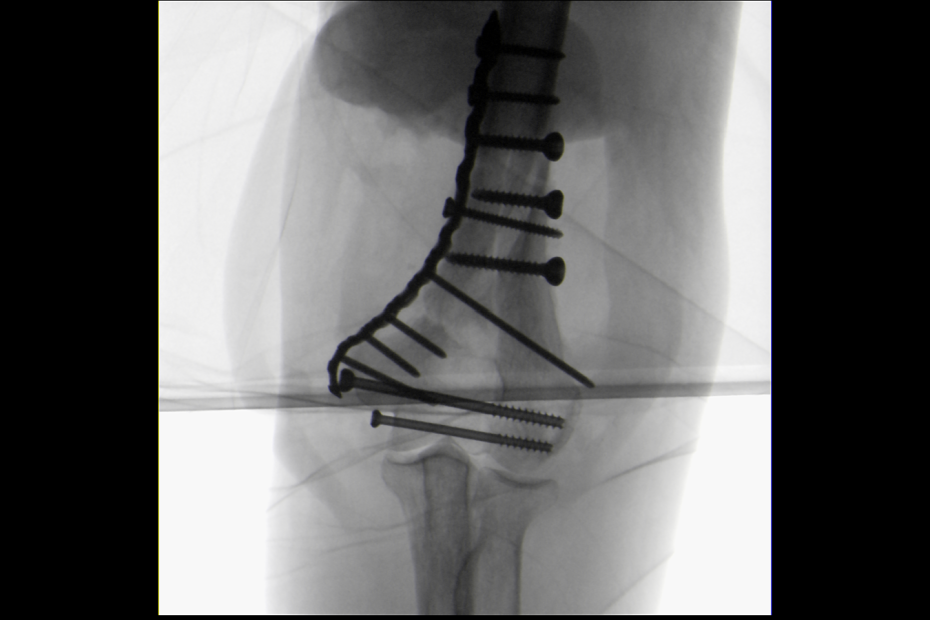
I operated on a young patient, an athlete with a rare comminuted fracture in the elbow joint (Fig. before). These injuries are very difficult to treat, as the fragments of the joint surface are often small and it is often not even technically possible to reassemble them.

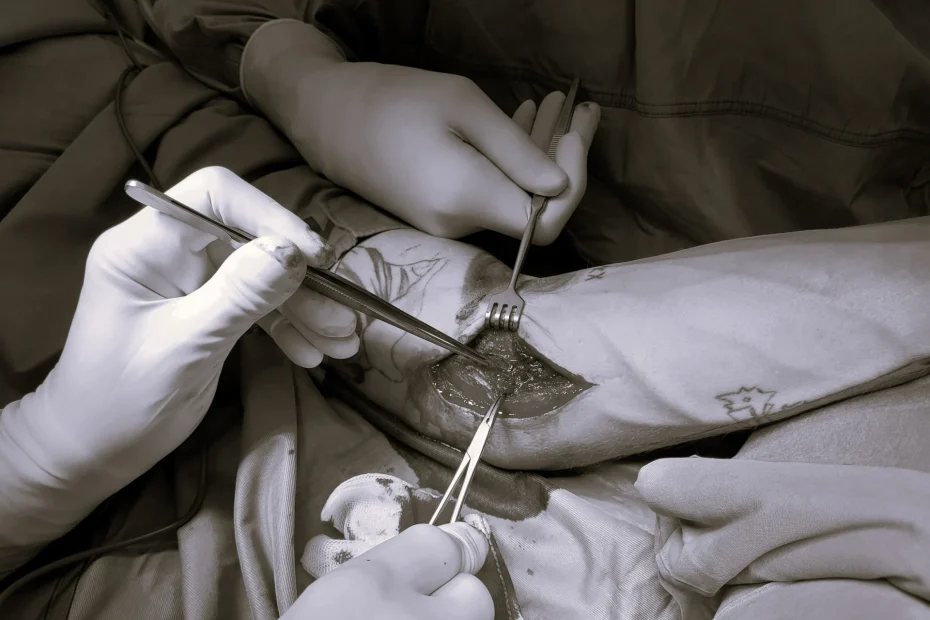
Today we operated on a very unstable elbow joint after a serious injury. We had to reconstruct both lateral ligaments and also the anterior joint capsule to restore the stability of the elbow. To ensure… Insights into an elbow surgery
A young athlete (pitcher in baseball) injured the medial collateral ligament of the elbow joint while pitching 3 years ago. He was treated in a specialized hospital by replacing the ligament with an artificial fiber.

I have now published my many years of experience with unhealed fractures of the lower end of the humerus and their solutions with the aid of artificial joints in the journal of the Austrian Society for Orthopedics and Orthopedic Surgery.
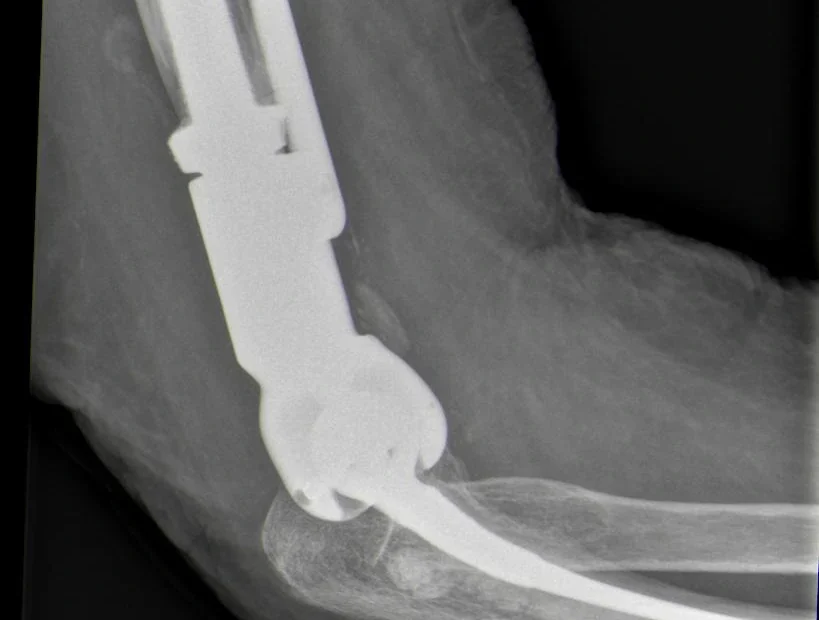
Surgery for an artificial elbow joint (endoprosthesis) is a complex procedure that is performed at only a few clinics. If an elbow arthroplasty is implanted in patients with an elbow fracture, the surgery is even more challenging.

In many patients, we encounter problems that arise from different areas at the same time. The most common are pain in the lumbar spine, buttocks and hip, and pain in the hip, knee and ankle.

Shoulder dislocation often also results in injury to the humerus or glenoid cavity. A defect (a dent) occurs in the posterior portion of the humeral head, and an anterior portion (of varying size) breaks away from the glenoid cavity of the scapula. If these injuries occur at the same time, the likelihood of the next shoulder dislocation is high.
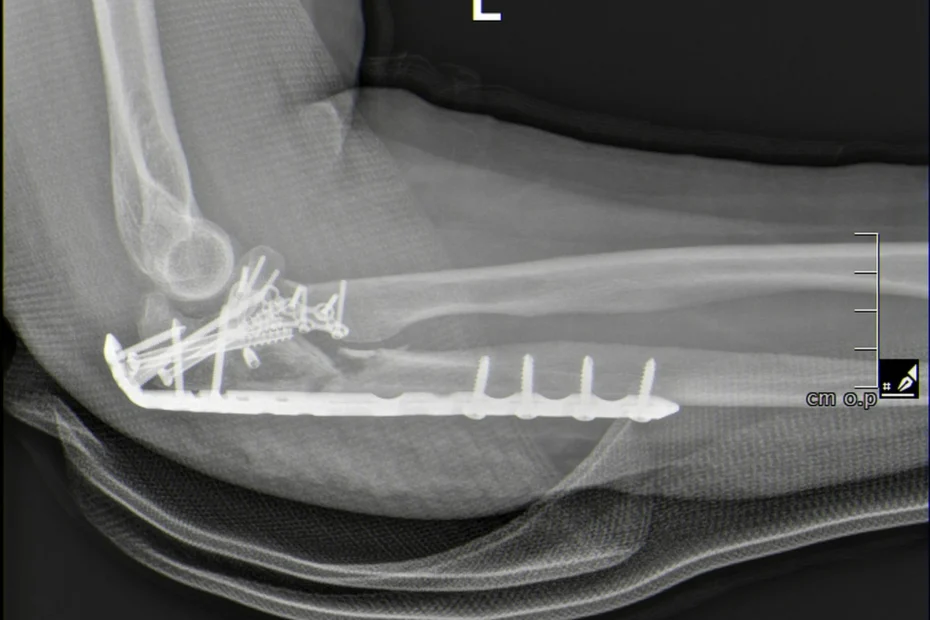
These are demanding procedures for the surgeon, which take 2.5 to 3 hours. The key to success in these cases is the correction of the ulna – reconstruction of its articular surface, restoration of its axis and length, and subsequent fitting with a plate. Then continue with the reconstruction of the upper end of the spoke.

In some cases, it certainly works! It is not uncommon to find axial deviations in the knee area in patients (more often in the form of the letter “O”, less frequently in the form of the letter “X”). If we align the limb axis in good time in these cases, we can either prevent the implantation of a total endoprosthesis altogether or at least delay it by many years.